
 Click here for Dental Services
Click here for Dental Services
![]() TRUE VALUE DENTAL INSTITUTE
TRUE VALUE DENTAL INSTITUTE
Blog By: Dr. Shivangi, True Value Dental Institute
Introduction
Covid-19 caused by SARS-CoV2 (Severe Acute Respiratory Syndrome- Coronavirus 2) majorly affects the respiratory system. The common signs and symptoms of SARS-CoV2 infection can be headache, sore throat, hyposmia, hyoguesia, diarrhea, dyspnea, and in severe cases pneumonia.1
Dermatologic implications include affected hands and feet in teenagers to vasculitis, rash, urticaria and varicella-like lesions.2
Since dentistry is the most prone profession in this pandemic, we need to take into consideration the oral manifestations of COVID-19 disease so that we can suspect the infection and get the possible confirmation tests done thereafter. Some oral conditions could be secondary to the deterioration of health due to other systemic diseases, opportunistic infections or due to the medication given during the treatment of COVID-19 disease.3
In this review article, we will discuss oral manifestations of COVID-19 disease and its similarity to commonly seen oral lesions.
Common Clinical Manifestations 4, 1
- Fever
- Nonproductive cough
- Sore throat
- Dyspnea
- Myalgia
- Fatigue
- Normal or decreased leukocyte counts
- Radiographic evidence of pneumonia.
- Cutaneous manifestations- mainly on trunk 5
- Erythematous rash
- Widespread urticarial
- Chickenpox-like vesicles
- Olfactory function impairment
- Hyposmia
- Organ dysfunction
- Shock
- Acute respiratory distress syndrome [ARDS]
- Acute cardiac injury
- Acute kidney injury
- Death-in severe cases
Why Covid-19 causes Oral manifestations?
Oral mucosa has been implicated as a potential route of entry for SARS-CoV-2.6
Viral load is the highest in the first week of COVID-19 disease, when the symptoms are generally mild.7, 8
Approximately 50% of the patients reported loss of taste.9, 10
At 48 h after intranasal viral challenges, viral loads of SARS-CoV were significantly higher in saliva than in blood samples.11These findings suggest that oral symptoms may occur due to impediment of salivary flow in these patients.
Why Tongue: Taste organs are widely distributed in oral tongue, where 96% of the oral ACE2-positive cells reside.12
Because of the angiotensin-converting enzyme 2 (ACE2) receptor, to which the SARS-CoV-2 binds (Fig. 1), in order to gain entry into the host cell, is highly expressed in the epithelial cells of especially the tongue, in comparison to the buccal or gingival tissues of the oral cavity.12
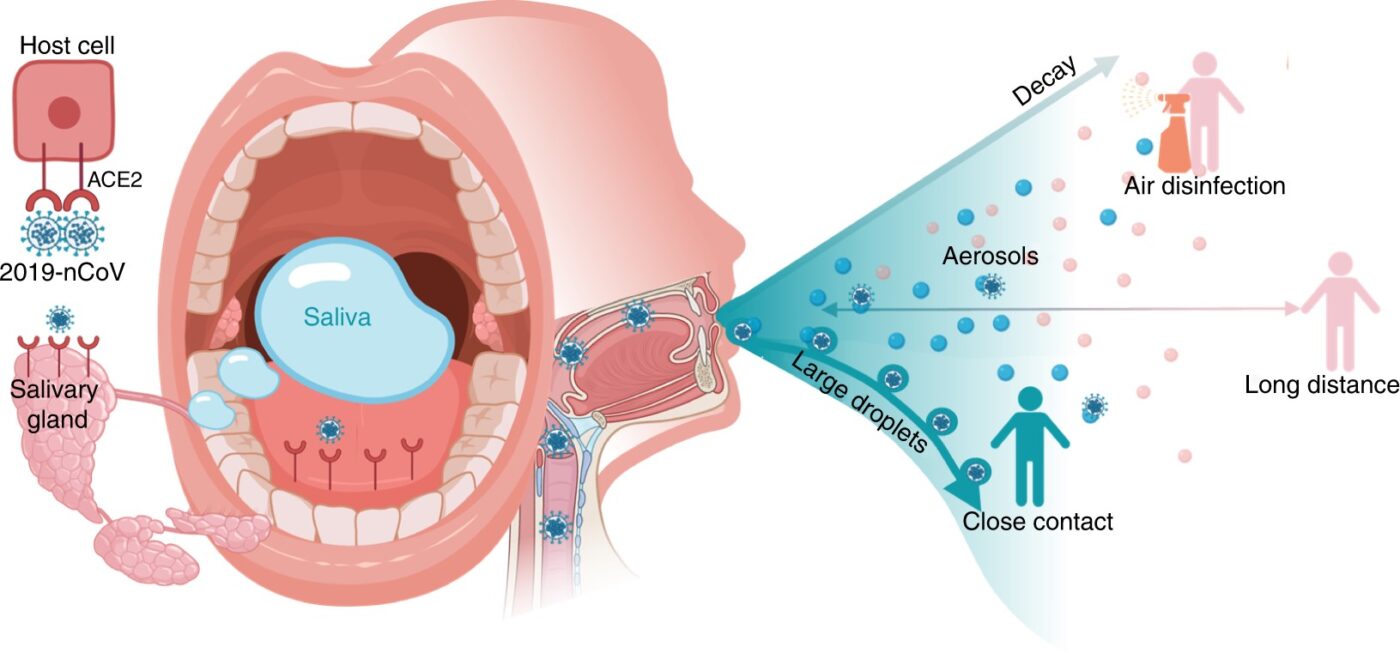
Figure 1: Potential diagnostic value of saliva and transmission of 2019-nCoV. Possibly combing to host-cell receptor of ACE2 expressed in salivary glands and tongue, 2019-nCoV is detected in saliva. Combined with infectious fluids from respiratory system, 2019-nCoV via large saliva droplets sets up short-distance transmission and hardly form long-distance aerosol transmission outdoors due to complicated physical and biological decay. Prevention of droplets formation, implementation of air disinfection, and blockage of droplets acquisition could possibly slowdown 2019-nCoV dissemination.13
Common Oral Symptoms
Can occur as early as first 24 hours of COVID-9 infection14 even before fever and cough occurs.15
- white plaque on tongue
- pain on hard palate and tongue
- ulcers on tongue14
- blisters on lip
- loss of taste
- dry mouth15
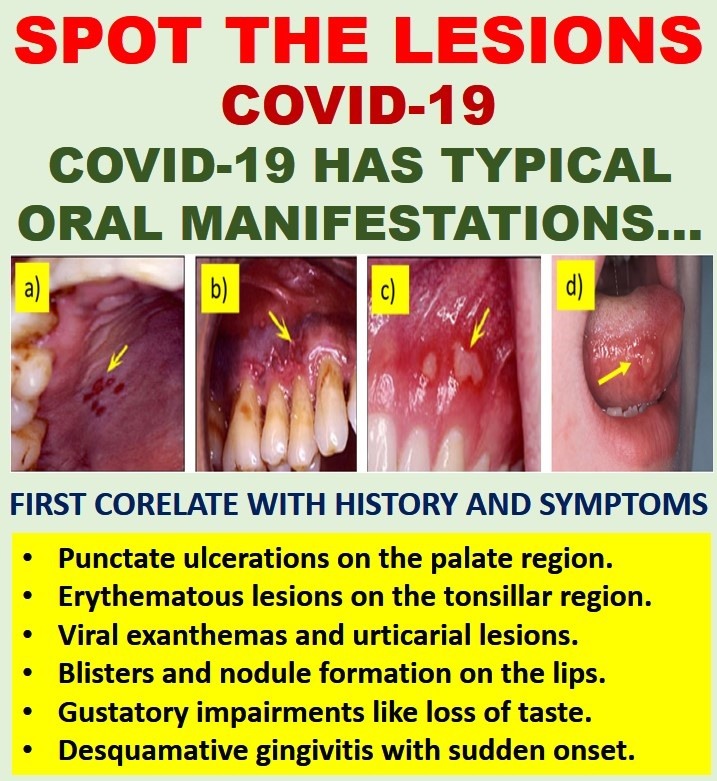
Common Oral Manifestations
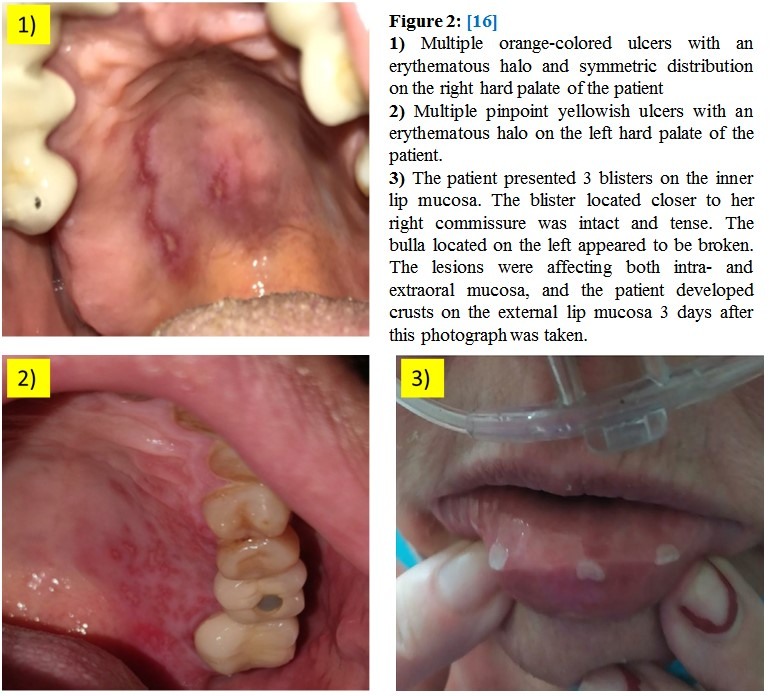
- Oral Ulcers and Blisters 3, 16
- Multiple orange colored ulcers with an erythematous halo (Fig. 2)
- Multiple pinpoint yellowish ulcers with an erythematous halo (Fig. 2 & Fig. 3)
- Blisters (Fig. 2) and nodule on the inside of lower lip.
- Desquamative gingivitis16
- Extremely viscous saliva
- Asymptomatic geographic tongue with sometimes a fissured tongue (Fig. 4)
- Slight erythematous area in palate region.3
- Viral exanthemas and urticarial lesions16(Fig. 5)
- Gustatory impairment17
- Dysgeusia and ageusia18
- Xerostomia15

Histopathology and Biopsy results
- Non-specific morphological findings with some suggestive of viral exanthema or urticariform dermatitis with discrete blood extravasation.
- Involvement of both keratinized and non-keratinized tissue.16
- Epithelium with severe vacuolization and occasional exocytosis. (Fig. 6)20
- A diffuse chronic inflammatory infiltrate associated with focal areas of necrosis and haemorrhage seen in the lamina propria.
- Evident thrombi obliterate conspicuous superficial and deep small vessels.
- Small thrombi seem to be composed mainly by endothelial cells, while the larger ones were composed by fibrin and endothelial cells. (Fig. 6)
- CD34 was positive for cells in the luminal component in either case. (Fig. 7)
- An intense lymphocytic infiltration, mostly positive for CD3 and CD8 exhibited in the adjacent minor salivary glands and in the basal layer of the epithelium. (Fig. 8)20
Healing of lesions on skin and oral mucosa
- Lesions heals within 7-10 days with symptomatic antiviral therapy and medication.
- Complete remission of lesions after 3 weeks of follow up.20
- No scar formation.
- No correlation with the severity of the disease.
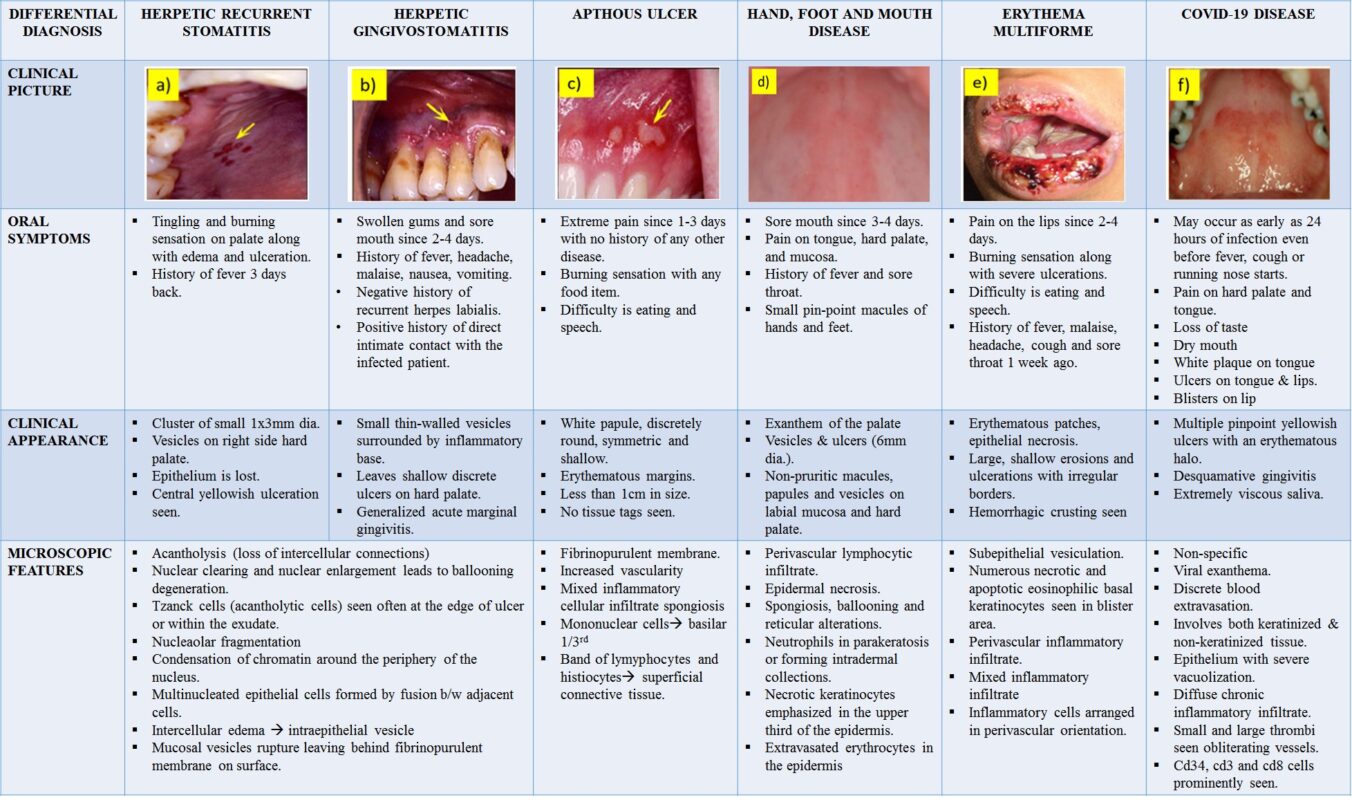
Differential Diagnosis (Table 1) 21
- Herpetic recurrent stomatitis
- Herpetic gingivostomatitis
- Apthous stomatitis
- Hand, food and mouth disease
- Erythema multiforme22, 2
Conclusion
In COVID-19 patients we should consider the occurrence of some oral signs and symptoms, including dysgeusia, petechiae, candidiasis, traumatic ulcers, HSV-1 infection, geographical tongue, thrush-like ulcers, among others. Thus, the importance of the clinical dental examination of patients with infectious diseases in the ICU should be emphasized, considering the need for support, pain control, and quality of life.3This might prevent the spread of the disease and immediate actions could be taken for the safety of the patient as well as the dentist.
In short, we suggest that SARS-COV-2 can cause oral lesions and therefore all patients positive for the virus should have a full mouth examination to better understand the pathobiology of these oral alterations.20

Figure 6: Clinical and Microscopic Features of Reddish Oral Lesions in a Patient with Covid-19. A: Diffuse reddish lesion in the hard palate. B: Ulcer with ischemic aspect in the buccal mucosa. C: Epithelium demonstrating vacuolization and haemorrhage in the superficial portion of the lamina propria, with hyperaemic vessels. D: Lymphocytic infiltration in the connective tissue and different-sized thrombi.

Figure 7: E: CD34 positive expression in thrombi of small vessels. F: Larger thrombi with variable amount of fibrin and endothelial cells positive for CD34.
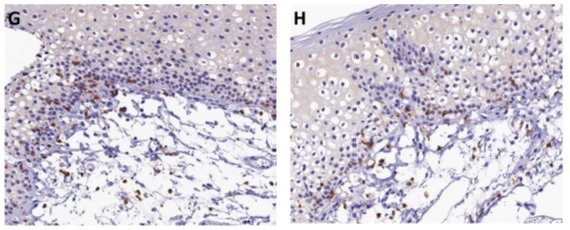
Figure 8: G: CD3 positivity in most inflammatory cells in the connective tissue and basal layer of the epithelium. H: CD8 highlighting lymphocytes in the lamina propria and basal layer of the epithelium.
Table 1: Differential Diagnosis for COVID-19 Disease 24-27
References
- Wang D, Hu BO, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA. 2020; 323(11), 1061. https://doi.org/10.1001/jama.2020.1585
- Estebanez A, Perez-Santiago L, Silva E, et al. Cutaneous manifestations in COVID- 19: A new contribution. JEADV. 2020. https://doi.org/10.1111/jdv.16474
- Santos JA, Normando AG, Silva RL, et al. Oral mucosal lesions in a COVID-19 patient: new signs or secondary manifestations? Int J Infect Dis. June 2020; 10.1016/j.ijid.2020.06.012
- Huang C,Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020 January 24; 10.1016/S0140-6736(20)30183-5
- Recalcati, S. Cutaneous manifestations in COVID-19: A first perspective. JEADV. 2020. https://doi.org/10.1111/jdv.16387.
- Peng X, Xu X, Li Y, Cheng L, Zhou X, Ren B.2020. Transmission routes of 2019-nCoV and controls in dental practice. Int J Oral Sci.12(1):9.
- To KK, Tsang OT, Leung WS, et al. 2020. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: an observational cohort study. Lancet Infect Dis [epub ahead of print 23 Mar 2020] in press. doi:10.1016/S1473-3099(20)30196-1.
- Wölfel R, Corman VM, Guggemos W, et al. Virological assessment of hospitalized patients with COVID-2019. Nature. 2020; 581:465–469. https://doi.org/10.1038/s41586-020-2196-x
- Chen L, Zhao J, Peng J, et al. Detection of 2019-nCoV in Saliva and Characterization of Oral Symptoms in COVID-19 Patients. 2020 March 14.. Available at SSRN: https://ssrn.com/abstract=3557140 or http://dx.doi.org/10.2139/ssrn.3557140
- Giacomelli A, Pezzati L, Conti F, Bernacchia D, Siano M, Oreni L, Rusconi S, Gervasoni C, Ridolfo AL, Rizzardini G, et al. 2020. Self-reported olfactory and taste disorders in SARS-CoV-2 patients: a cross-sectional study. Clin Infect Dis [epub ahead of print 26 Mar 2020] in press. doi:10.1093/cid/ciaa330
- Liu L, Wei Q, Alvarez X, Wang H, Du Y, Zhu H, Jiang H, Zhou J, Lam P, Zhang L, et al. 2011. Epithelial cells lining salivary gland ducts are early target cells of severe acute respiratory syndrome coronavirus infection in the upper respiratory tracts of rhesus macaques. J Virol. 85(8):4025–4030.
- Xu H, Zhong L, Deng J, et al. High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. Int J Oral Sci. 2020; 12(8).
- Xu R, Cui B, Duan X, et al. Saliva: potential diagnostic value and transmission of 2019-nCoV. Int J Oral Sci 12, 2020;11. https://doi.org/10.1038/s41368-020-0080-z
- Chaux-Bodard AG, Deneuve S, Desoutter A. Oral manifestation of Covid-19 as an inaugural symptom? J Oral Med Oral Surg. 2020 April12;26:18.
- Ren YF, Rasubala L, Malmstrom H, et al. Dental care and oral health under the clouds of COVID-19. JDR Clinical & Translational Research. 2020. DOI: 10.1177/2380084420924385
- Martín Carreras-Presas C, Amaro Sánchez J, López-Sánchez AF, et al. Oral vesiculobullous lesions associated with SARS-CoV-2 infection. Oral Dis. 2020.May 5; 10.1111/odi.13382
- Vinaychandran D, Balasubramanian S. Is gustatory impairment the first report of an oral manifestation in COVID-19? Oral Dis. 2020 May 18; 10.1111/odi.13371
- Matsuo R. Role of saliva in the maintenance of taste sensitivity. Critical Reviews in Oral Biology & Medicine. 2000; 11(2), 216–229. https://doi.org/10.1177/10454 41100 01100 20501
- Picciani BLS, Santos LR, Teixeira-Souza T, et al. Geographic tongue severity index: A new and clinical scoring system. Oral Surg Oral Med Oral Pathol Oral Radiol. 2020;129(4):330‐338. doi:10.1016/j.oooo.2019.12.007.
- Soares CD, Carvalho RAd, Carvalho KAd, Carvalho MGFd, Almeida OPd. Oral lesions in a patient with Covid-19. Med Oral Patol Oral Cir Bucal. 2020 Jul 1;25 (4):e563-4.
- Scully C, Samaranayake LP. Emerging and changing viral diseases in the new millennium. Oral Diseases. 2016; 22(3), 171–179. https://doi.org/10.1111/odi.12356
- Trayes KP, Love G, Studdiford JS. Erythema multiforme: Recognition and management. American Family Physician. 2019; 100(2), 82–88.
- Schwartz RA, Janniger C.K. Generalized pustular figurate erythema: A newly delineated severe cutaneous drug reaction linked with hydroxychloroquine. Dermatologic Therapy. 2020; e13380, 1–3.https://doi.org/10.1111/dth.13380
- Burket LW, Greenberg MS, Glick M. Burket’s oral medicine: Diagnosis & treatment. Hamilton, Ont: BC Decker. 2003; 10:50-84.
- Tilliss TS, McDowell JD. Differential diagnosis: Is it herpes or apthous? J Contemp Dent Pract. 2002 Feb 15; 3(1): 1-15.
- Böer-Auer A, Metze D. Histopathology of Hand-Foot-Mouth Disease in Adults and Criteria for Differentiation From Erythema Multiforme. Am J Dermatopathol. 2019;41(4):273-280. doi:10.1097/DAD.0000000000001263
- Joseph TI, Vargheese G, George D, et al. Drug induced oral erythema multiforme: A rare and less recognized variant of erythema multiforme. J Oral Maxillofac Pathol. 2012 Jan-Apr; 16(1): 145–148.
Dr. Shivangi
Research Team
TRUE VALUE DENTAL INSTITUE
Email: truevaluedentalinstitute@gmail.com
Available from: www.truevaluedentalinstitute.com
| Courses, careers, mission abroad, placements, practice setup |
Very well explained. For all dentists. It’s good for differential diagnostics and good for prevention.
Very well explained. For all dentists. It’s good for differential diagnostics,prevention.